 via healthpopuli.com
via healthpopuli.com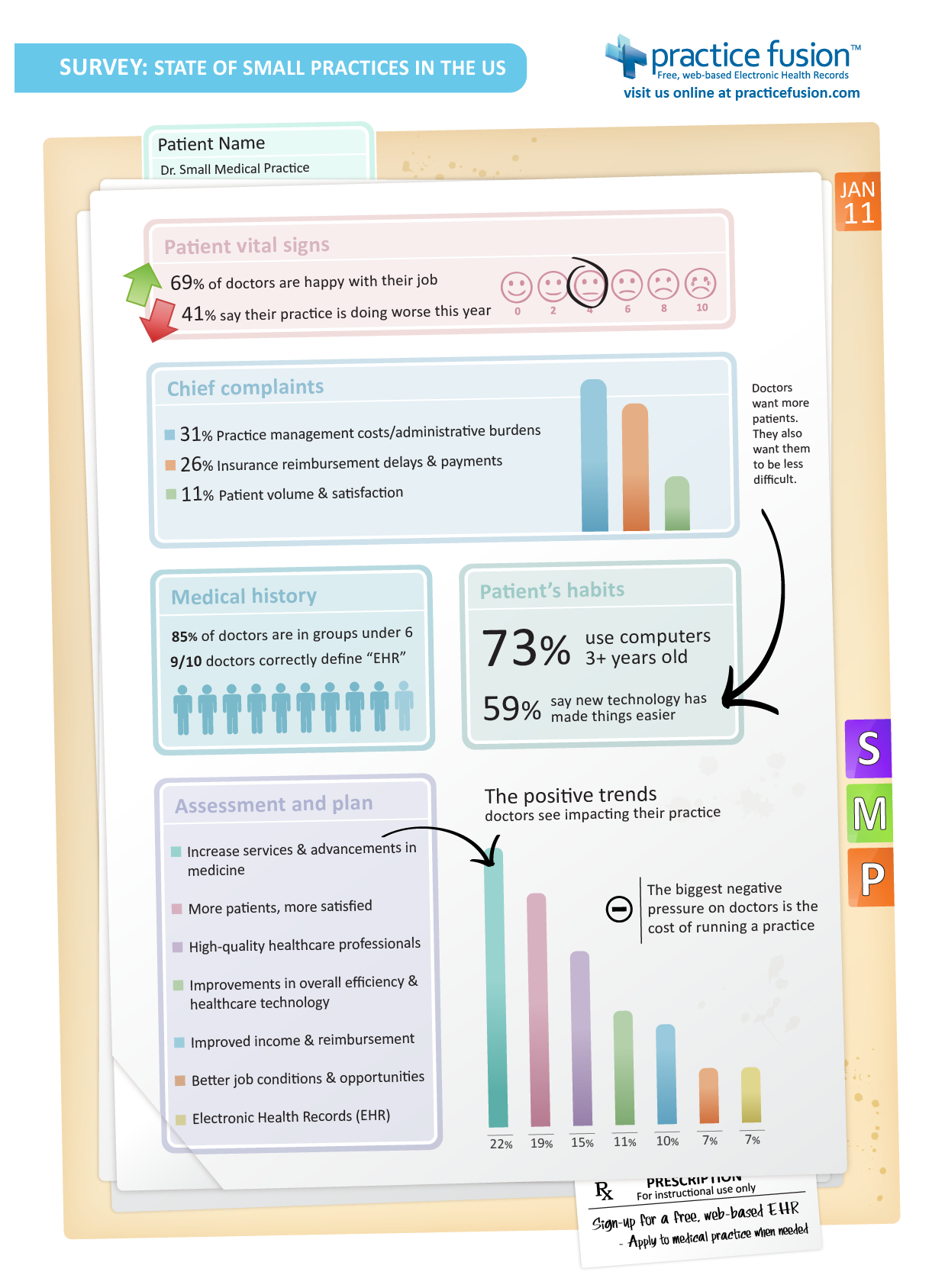{kind=link}
What a revealing graphic. Practice Fusion continues to impress.
 Patients being non-compliant with taking their medication negates the value of going to the doctor, creates confusion in setting up treatment plans and in the case of antibiotics teaches the exact bacteria you're trying to kill how to fight back (MRSA).
Patients being non-compliant with taking their medication negates the value of going to the doctor, creates confusion in setting up treatment plans and in the case of antibiotics teaches the exact bacteria you're trying to kill how to fight back (MRSA)....the Zuri, an iPod-sized device that sends patients reminders to take their medications and records their compliance, which users and, if they choose, their doctors can track through a companion Web page.
Intel's care-management tool, called Health Guide, combines an in-home patient device with an online interface that doctors can use to monitor and remotely manage care. The in-home patient device collects readings from specific models of wired and wireless medical devices, such as blood-pressure monitors and glucose meters. It then displays the data for the patient on a touch screen and sends the readings to a secure host server, where health-care professionals can review the information and provide feedback via video conferencing and email.
Meanwhile, Microsoft is working with home-health and fitness-device makers to integrate vital-signs data into HealthVault, an online service the software company recently launched that allows consumers to store, manage and selectively share medical data.
"Keeping [at-risk] patients stable and quickly getting them care when it's needed can reduce hospitalizations and cut the insurer's medical costs. And since the savings come from improving the patient's health and quality of life, programs such as Blue Cross' "Your Heart Matters" are generally popular with participants."That's from this article detailing how the above congestive heart failure (CHF) program works remotely from patient's homes.
"Every morning, Sedaris steps on a special digital scale beside the bed in her Raleigh home and answers a series of questions. Is she swollen or short of breath? Has she taken her medicines? The scale, provided by her health insurer, ships her weight and other data to a nurse's computer at Blue Cross and Blue Shield's disease management center in Winston-Salem. Any suspicious results -- an overnight weight gain of just a pound or two is a signal that Sedaris is retaining fluid that may strain her heart -- and the nurse is on the phone. She'll talk with Sedaris and, if necessary, send her to get medical attention.This is incredible! For more, here's another personal example from the Healthcare Economist.
The technology to remotely monitor patients' pulse, weight, blood pressure, blood-oxygen levels, general mobility and other indicators is already widely available. The declining costs and increasing use of high-speed Internet service should only accelerate acceptance of monitoring devices."
"On the doctor side, I have a facebook-like platform that allows me to see and receive client updates and communicate via email, IM, video, and SMS with my clients and colleagues. We don’t do eVisits — we simply communicate normally via a whole range of communication options to help streamline healthcare delivery."Hello Health!
 "Tethered" means linked only to a provider or a hospital and "standalone" refers to a web-based service like WebMD or Microsoft's HealthVault. Its hard to build a Facebook, let alone a medically-based version with all the privacy/security issues involved. The need is obviously there. PHRs won't take off without it.
"Tethered" means linked only to a provider or a hospital and "standalone" refers to a web-based service like WebMD or Microsoft's HealthVault. Its hard to build a Facebook, let alone a medically-based version with all the privacy/security issues involved. The need is obviously there. PHRs won't take off without it.Have you noticed how the word, "vista" has been popping up everywhere?? Considering definition #3, I understand why and it makes even more sense in the corporate view of things. Strategic planning meets Marketing, right? Here are a few more instances:Vista (vist-uh) n.
1. a view or prospect, esp. one seen through a long, narrow avenue or passage, as between rows of trees or houses.
2. such an avenue or passage, esp. when formally planned.
3. a far-reaching mental view: vistas of the future.
"Consumption is the sole end and purpose of all production; and the interest of the producer ought to be attended to, only so far as it may be necessary for promoting that of the consumer."Carol is a health care marketplace that basically allows you to purchase care packages for what you need. Say you have a sore throat and you're worried it might be something worse. Using Carol's body chart, you click on the throat region, scroll down to sore throat and click on the test, treatment or procedure that most suits your condition. In this case, the options are mononucleosis (mono) symptoms: evaluation & treatment and sore throat: evaluation & management. Clicking on the latter leads to a "compare care packages" page where you can select a vendor based on price and facility.
--Adam Smith
"To say that the backdrop is 'recession like' is akin to an obstetrician telling a woman that she is 'sort of pregnant'," the report said.Got it. Most people do think we're headed towards some sort of downturn though. A definition is appropriate here :
The NBER defines a recession as "a significant decline in economic activity spread across the economy, lasting more than a few months".It bases its assessment on final figures on employment, personal income, industrial production and sales activity in the manufacturing and retail sectors.
Are you a butcher? Set your SnūzNLūz to donate to PETA
Are you a republican? Set your SnūzNLūz to donate to the ACLU!
"SEC staff have been working on a proposal for “mutual recognition” between the SEC and other regulators that would allow the US watchdog to rely on foreign regulators’ standards as US investors trade abroad...There is a huge demand for this type of service:
...As part of the new SEC approach, a foreign exchange would be allowed to install a trading facility on the desk of a US broker, provided that the exchages’ home-country regulators’ rules were deemed “comparable” to the SEC’s."
The odd thing to note here is that while you must interface first before you can interoperate, the demand for interoperability - the desire for culture change - is what leads to interfacing - the desire to speak the same language."The policy shift, backed by SEC chairman Christopher Cox, has been prompted by the increasing appetite of US investors for foreign securities.
Nearly two-thirds of American investors have holdings in non-US companies, a 30 per cent increase from five years ago."
iHealthBeat recently featured an article called, "DrTube: Physicians Tap Online Video To Communicate With Patients". Click on the link to directly view it.
The paradigm shift in physician thinking from independent contractor to entrepreneur is a key point in the article. Connecting with patients on their level, assessing demand for services and supplying to that demand in simple terms is basic marketing but a relatively new concept in modern medicine.
Here's the bottomline:
 HealthVault lets you share your "strong" password with other providers of your choice, but what happens when you move or don't want to see that provider anymore? Do you have to change your password everytime?
HealthVault lets you share your "strong" password with other providers of your choice, but what happens when you move or don't want to see that provider anymore? Do you have to change your password everytime?